
If the Regency period conjures images of elegance and refinement, it’s worth remembering that everyday life told a rather different story, particularly when it came to health and illness. Behind the polished social world lay a system of care that was uncertain, uneven, and deeply shaped by circumstance. In this post, I explore what that really meant for ordinary people, and how their experiences of sickness and care were woven into the fabric of daily life.
To understand healthcare in the Regency era, you have to appreciate the broader context. Britain at the time was undergoing significant social and economic change: urban populations were swelling due to early industrialisation, yet infrastructure hadn’t caught up. Overcrowded housing, poor drainage, and limited access to clean water created ideal conditions for disease to spread. At the same time, medicine had not yet undergone the scientific revolution that would transform it later in the 19th century.

At the heart of Regency medicine was a theoretical framework that had persisted for centuries: the theory of the four humours. This idea, originating in ancient Greece, proposed that the body was governed by four fluids: blood, phlegm, black bile, and yellow bile; and that illness resulted from an imbalance among them. It wasn’t just a vague notion; it actively shaped diagnosis and treatment. A fever might be interpreted as an excess of blood, while lethargy could be blamed on too much phlegm. Treatments, therefore, aimed to restore balance, often by removing what was thought to be the offending substance. Bloodletting was the most dramatic example, carried out using lancets or leeches, sometimes in alarming quantities. It persisted not because it worked in any meaningful sense, but because it fit neatly within the prevailing logic of the time, and occasionally, by sheer coincidence, patients survived.
Behind such treatments lay healthcare professions carefully structured around hierarchy and social distinction, reflecting a deeply stratified society. Physicians occupied the top tier. They were university educated, typically at Oxford or Cambridge, and approached medicine as a learned, almost philosophical discipline. They diagnosed illness, advised on treatment, and enjoyed considerable social prestige, but often had limited hands-on involvement. Surgeons, by contrast, had more practical training and were responsible for procedures such as amputations, setting fractures, and treating wounds. Their historical association with barbering is not merely a quirky footnote; it speaks to their more manual, less prestigious status. Apothecaries filled an essential middle ground. They prepared and sold medicines, but increasingly took on the role of diagnosing and treating patients, particularly among the middle and lower classes. In many ways, they were the most accessible practitioners, though their training varied widely.
In the Regency period, the role of the “nurse” also existed, but it was loosely defined, inconsistently practised, and carried very little of the professional identity we attach to it now. There was no formal training, no regulatory body, and certainly no standardised expectation of care. The transformation of nursing into a trained, respected profession didn’t begin until later in the 19th century, most notably with figures like Florence Nightingale. Her work during the Crimean War (1850s) and subsequent reforms introduced the idea that nursing required education, discipline, and a scientific approach. That shift was still decades away during the Regency period. Nursing at the time was typically seen as domestic or menial work rather than a skilled discipline, and those who undertook it were often from the lower social classes. In many cases, nursing roles were filled by women who had few other employment options.
These attitudes to nursing were closely tied to how hospitals themselves were organised and accessed. Hospitals were not the centres of healing we might imagine today. They were relatively scarce and primarily served the poor, funded by charitable donations. Admission was often conditional, requiring a letter of recommendation from a subscriber, which rather neatly ensured that even charity came with a layer of social gatekeeping. Inside, conditions could be grim. Wards were crowded, ventilation was poor, and there was no understanding of infection control. Surgical instruments were reused without sterilisation, and staff moved between patients without any form of hand hygiene. Unsurprisingly, hospitals could become hotspots for disease rather than places of recovery.
Nurses were responsible for the basic care of patients in hospitals. This included tasks like washing, feeding, changing linens, and maintaining the ward environment. It’s worth noting that the reputation of hospital nurses during this period was, frankly, not stellar. Contemporary accounts often describe them as untrained, rough, and sometimes neglectful. Some were known to drink on duty or prioritise convenience over patient comfort. However, it’s important to remember the conditions they were working in: long hours, minimal pay, little oversight, and no real education.
Outside hospitals, nursing looked quite different. Most care actually took place in the home, particularly for those who could afford it. Families, especially women, were the primary caregivers. Wives, mothers, and daughters took on the role of nurse for sick relatives, drawing on a mixture of practical experience, folk knowledge, and whatever medical advice they could access. In wealthier households, a hired nurse might be brought in, particularly for childbirth or serious illness. These nurses varied widely in competence; some were experienced and highly regarded, others… less so.

It is within this domestic, largely female-led sphere of care that one of the most significant and perilous aspects of Regency healthcare unfolded: childbirth. Maternal mortality in England during this period is estimated at roughly 1–1.5% per birth, a sobering figure when you considers the number of pregnancies many women endured. Most births took place at home under the care of a midwife, many of whom were experienced and respected within their communities. However, they lacked access to effective interventions for complications. Conditions such as obstructed labour, eclampsia, or postpartum haemorrhage were often fatal. When complications arose, a physician or surgeon might be called, sometimes bringing instruments such as forceps. While these could be life-saving in certain cases, they also carried significant risks, especially in an era without anaesthesia or antiseptic practice. Puerperal fever (postpartum infection) was a significant cause of death, though its transmission would not be properly understood until the work of Ignaz Semmelweis later in the century. Maternal mortality rates were high, and infant survival was far from guaranteed. It’s one of those areas where the gap between then and now feels particularly profound.
Childcare and “nursing” infants was another important aspect of the nursing role. Wet nurses were commonly employed by wealthier families to breastfeed and care for babies. This was a socially accepted practice, though it came with its own risks, including the transmission of disease and the emotional separation between mother and child. Again, it highlights how the concept of nursing was tied as much to domestic service as to healthcare.
Within this blending of domestic caregiving with early forms of medical intervention, we find the wider range of therapeutic practices used to manage illness. Treatments during this period ranged from the genuinely useful to the deeply questionable. Herbal medicine had a long tradition, and some remedies, such as those derived from willow bark (a precursor to aspirin), did have real effects. However, many treatments were based more on tradition than evidence. Laudanum, a widely used opium-based tincture, was prescribed for pain, insomnia, diarrhoea, and even minor complaints. Its effectiveness in dulling symptoms made it popular, but its addictive nature was not well understood. Mercury, used in the treatment of syphilis, is perhaps the most notorious example of a harmful remedy. Patients often endured severe side effects, including neurological damage, in the hope of a cure that was far from guaranteed.

Alongside these physical treatments, there was also a growing, though still very limited, attempt to grapple with conditions affecting the mind, where medical understanding was even more tentative and responses reflected a similarly uncertain blend of theory and practice. Mental illness was increasingly medicalised during this period, but treatment remained rudimentary. Institutions like the Bethlem Royal Hospital housed patients under conditions that varied widely. Some reforms were underway, particularly the “moral treatment” movement, which advocated humane care, but progress was uneven. Public attitudes often mixed fear, curiosity, and misunderstanding, and stigma was widespread.
While the treatment of mental health revealed the limits of contemporary understanding in one direction, infectious disease represented the most pervasive and immediate challenge to life in the Regency period, shaping everyday mortality on a far broader scale. Infectious diseases, particularly smallpox, tuberculosis (often referred to as consumption), typhus, and cholera were widespread and frequently fatal. The lack of understanding about how diseases spread meant that preventative measures were limited. Contaminated water supplies, poor sanitation, and close living quarters all contributed to repeated outbreaks.
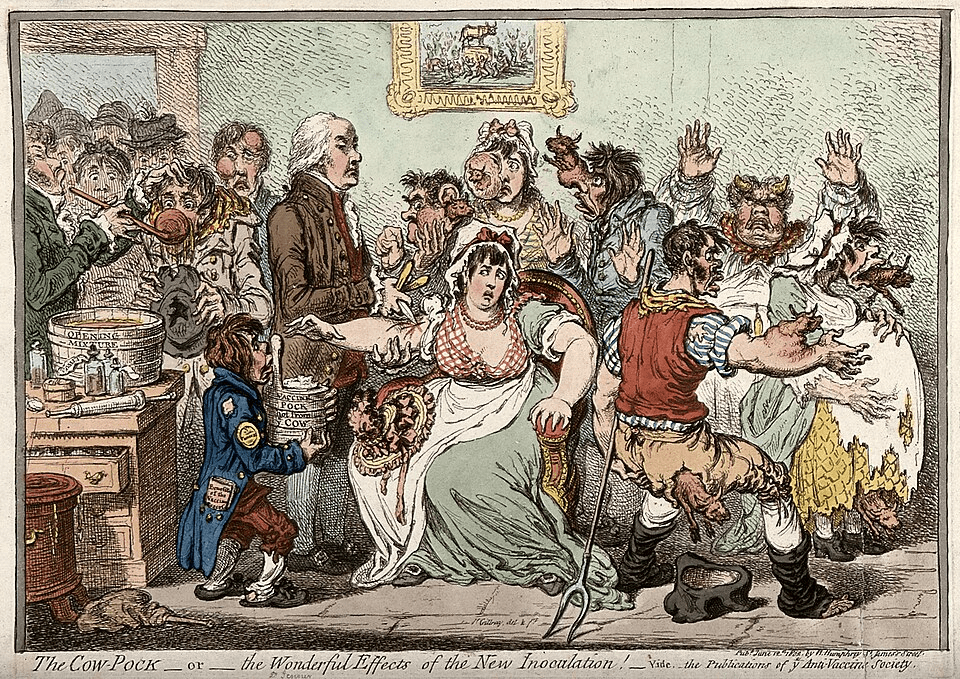
By the early 19th century, inoculation, and increasingly vaccination, was becoming more common, following the work of Edward Jenner. His development of the smallpox vaccine in 1796 marked a turning point, offering a level of protection that was revolutionary for its time.
While smallpox vaccination offered an early glimpse of what targeted prevention could achieve, most other diseases remained largely untouched by effective intervention, leaving broader population health to be shaped far more by environment and infrastructure than by medical treatment. Organised public health systems were still very much in their infancy, and the rapid pace of urbanisation during the Industrial Revolution only intensified the problem, as growing city populations were often housed in overcrowded conditions with limited infrastructure to support them, thereby creating an environment in which disease could spread with relative ease. Clean water supplies, sewage systems, and waste management were, at best, inconsistent and poorly coordinated, meaning that basic sanitation, which we now take for granted, was far from reliably available across urban areas. It was not until later in the 19th century, particularly in response to repeated cholera outbreaks, that large-scale public health reforms began to emerge in a more systematic and sustained way.
Despite these challenges, the Regency period was not entirely devoid of progress. There was a growing interest in anatomy and medical education, with dissections becoming more common (although cadavers were sometimes controversially sourced…). Medical texts were being published and circulated more widely, and some practitioners began to question traditional theories. These shifts, while gradual, signalled the beginning of a transition towards a more scientific approach to medicine. The real breakthroughs – anaesthesia in the 1840s; antiseptic techniques in the 1860s – were still to come, but the groundwork was being laid.
Stepping back from the detail, a broader picture begins to emerge. This is not a story of ignorance so much as a world trying (often imperfectly, sometimes disastrously) to make sense of human illness with the tools it had available. Regency healthcare sat at the intersection of long-standing belief systems, emerging scientific curiosity, and deeply uneven social structures, meaning that where you lived, what you earned, and who you were all mattered just as much as the illness itself. For those tracing family histories, it is a useful reminder that the names in parish records were not just entries in a ledger, but people navigating childbirth without anaesthesia, infectious disease without understanding of contagion, and treatments that could as easily harm as heal. Seen in that light, the Regency period becomes less a backdrop of elegant nostalgia and more a landscape of resilience, uncertainty, and quiet endurance, one that sits just beneath the surface of so many ancestral stories.






Comments, insights, and gentle corrections welcome.